

“I don’t think you are doing that right…” Equipment selection and use in CBRN Operations: Part 2
[Above photo: An Army Reserve CBRN specialist checks artillery rounds for radiation levels at Dugway Proving Ground during a validation event. (Source: dvidshub.net, US Army Reserve 76th Operational Response Command, Photo by SFC Brent Powel)]
The Basic Kit: Monitoring for Radiation
Introduction
In my previous post, I discussed some of the unit challenges of equipment selection and use in CBRN operations as it related to Personal Protective Equipment (PPE) and introduced the idea of “Personal Safety” equipment as part of a CBRN operator’s basic kit for most/all missions. This series builds off of the ideas I’ve written about previously as part of a target-based approach to CBRN operations, see here:
An Alternate Approach to CBRN Operations
Following Captain Obvious: A guide to CBRN operations against obvious targets
Don’t Break the Beaker: CBRN Operations Against Small Scale Production Facilities and Laboratories
CBRN Operations and Industrial Scale Production/State-Sponsored Programs
Proving the Negative and Cleaned Sites
To review, the basic “personal safety” kit for CBRN operators consists of:
An adequate level of PPE (see the previous post for a full discussion)
A gamma/neutron radiation monitor and dosimeter (might be one instrument or two separate devices – active and passive)
An air monitoring instrument for confined spaces
A personal chemical agent detector/alarm (Optional, depending on mission requirements)
In this post, I’m going to take a deep dive on radiation monitors/dosimetry and look at ways CBRN operators use and misuse radiation monitors and dosimeters and explore the concept of radiation monitoring, safety, and dosimetry in the context of actual hotzone entry/operations.
Radiation Doses, Dose Rates, and Operational Exposure Guidelines
Suspecting the presence of radiation can occur through direct observation (radiation markings, shipping containers, lead or other shielding material or pigs, labels, etc.), but the only way to detect radiation with any confidence is with the use of specialized detection equipment. Unless your mission profile expects radioactive material, it is usually not necessary to carry radiation detection equipment into the hotzone, beyond a personal alarm – an AN/UDR-13, radiation “pager,” or another device – a personal protective detector.[1] That does not mean the team may not bring more advanced point radiation detectors (to include those for alpha/beta or neutron radiation) or radioisotope identification devices, only that they may not bring them on initial entry into a CBRN target if the mission profile does not include a known or presumed radiation risk.
The reason to always carry a radiation monitor/alarm is twofold: first, they are small, easy to use, clip to a belt/uniform/vest and do not require constant monitoring or manipulation; second, radiation sources pop up in weird places. The first is self-evident, carrying a personal radiation detector/alarm is a no brainer that adds little to operator load. The second is less so and not always one CBRN operators think about, especially if they lack field and operational experience.
During operations in Iraq, there were many instances where radioactive material looted during the 2003/2004 period cropped up in unusual places, from ruined Former Regime facilities to chemists’ shops in the souks, or among medical supplies in abandoned, looted, or damaged hospitals and other medical facilities. There was also concern regarding radioactive material in old lightning rods and more than a few non-destructive testing devices and x-ray inspection cameras from the oil and pipeline industry in Iraq went missing or showed up in scrap heaps, black markets, or other unusual places. Medical isotopes found their way into all sorts of places with all kinds of people (usually unaware of the risks they posed to them). I came across several random sources myself, each time unexpected and found by accident when our UDR-13 alarms went off.
The truth is, radiation can pop up anywhere on a battlefield or in CBRN operations and its presence in a lab, industrial facility, medical facility or anywhere else is not as unusual as many believe, especially where there are oil and gas exploration and refining activities, pipelines, or non-destructive testing of aircraft, buildings, pipes, or other materials, and in most research facilities (in other words - everywhere). The only way to detect the presence of many of these radiation sources is with a personal monitoring device. Without it, many of the sources and dangers are undetectable, until it is too late.
Operation of personal radiation detection devices is simple, but there are several vital points that operators sometimes overlook. The first is where to set the alarm. Three to five times background is usually a good rule of thumb. However, operators must be aware of factors that may cause them to have to change their settings and incorporate procedures into their Standard Operating Procedures (SOP) to evaluate their settings and under what conditions.
For example, if an operation sets out low elevation and hits a target high in the mountains, the change in background radiation due to variation in altitude or because of the presence of naturally occurring radiation (NORM) in rocks at the target, will set off alarms that were set three times background at the low elevation. Therefore, before hitting a CBRN target, it is usually wise to take a glance at the background reading in the vicinity of the target and assess if it is a significant change from “base” levels recorded before hitting the Line of Departure (LOD) for the mission. If levels are higher (or lower), operators should adjust their alarms accordingly, unless there is a reason to suggest that the higher level is not a natural phenomenon.
Remember, the purpose of a three times background alarm is to alert an operator of the unexpected presence of a gamma-emitting radioactive source, not every minor change in the background radiation, which can fluctuate in strange ways. In one building where I worked, the bricks emitted a low level of radiation just above 3 times background in the area that would set off personal detectors whenever you leaned against the wall (reducing the distance to the source and therefore increasing the dose/dose rate) – the cause, an elevated NORM in the material used to make the bricks.
The second primary consideration related to Personal Protective Detectors (PPD) for radiation relates to targets where the team expects to encounter radiation. A setting of three times background in these scenarios is going to set off all the alarms as soon as you are on target! If you are assessing a research reactor, for example, the radiation levels will be much higher than three times background, even with the presence of thick concrete and water shielding around the source material.
If the reactor is operating, you will also see your neutron detector (if you have one) light up and start pinging. The same is true in situations where there is extensive radiation contamination: Radioactive Material Dispersal Devices (RDDs) or so-called dirty bombs, nuclear or radioactive material accidents or transportation incidents, and disasters involving radioactive material or nuclear reactors. At the extreme end, CBRN operators may encounter nuclear weapons detonations, testing, or criticality incidents related to enrichment or core milling/production activities.
In situations where an operator expects radiation, they should set personal alarms according to pre-established turn back doses. Here again, there are often misunderstandings. Military CBRN operators should not use the dose limits typically found in older military doctrine related to nuclear weapons and a nuclear battlefield! Those exposure limits set levels at which military units can continue to operate on a nuclear battlefield for the short term without significant health effects. The key is “short term” – military effectiveness measured in days or weeks does not equate with lower cancer/death rates in the longer term!
During Operation Iraqi Freedom, many CBRN officers set exposure limits for radiation using those Cold War levels, failing to understand the consequences and the lack of necessity to do so. In the early years of Operation Iraqi Freedom, I saw numerous operations orders that specified radiation dose limits of 40 rem - a ridiculously elevated level considering the actual threat. Since then, Joint Doctrine revised the recommended operations levels to more reasonable levels (see below), but many misunderstandings remain, and the newer guidance is confusing, especially for the uninformed.
It is best, short of nuclear conflict, to use the levels set by the US Environmental Protection Agency (EPA) or equivalent organization (depending on your country of origin) or follow the Joint US doctrine or NATO doctrine that incorporates those guidelines. Now, there are some debates about some of these levels, mainly that they are too low for emergency response and public protection in a significant incident. There is validity in those arguments and EPA did adjust its guidance recently in that regard, especially when it comes to public protection levels in the wake of a nuclear accident (a very controversial and much-debated topic I’m going to save for another day).[2] However, when in doubt, follow applicable national guidance or military doctrine (I’ve helpfully linked to some of these later in this article).
Now, before delving into some basics regarding dose alarms, we need to define a few things:
Occupational Dose Limit – this is a regulatory defined limit and translates to how much exposure radiation workers can receive during 8-hour days/40-hour weeks over the course of a year with no ill health effects. Given the occupational limit of 5 rem, that’s the total for the entire year for most “workers” under the NRC regulation, though it’s a bit more granular: under NRC regulations (10 CFR 20.1201) the annual limit is a total effective dose equivalent of 5 rem (0.05 Sv), with more specific dose limits for the eyes (15 rem), skin/shallow dose (i.e., alpha/beta - 50 rem), and extremities (50 rem).
Acute Dose Limits – these are single, one-time exposure limits (usually less than an hour).
Lifetime limits – these are the maximum lifetime limits, which implies you are tracking such things, something not always done well, even by CBRN professionals. The only places that do a good job of monitoring these are nuclear facilities regulated by the NRC, NNSA, or otherwise subject to IAEA guidelines or other national regulatory oversight. Dose tracking is an area where a lot of CBRN and response units need improvement.
Dose rate – A limit of how much radiation an individual is receiving in a set period (usually an hour) measured in a variety of ways: rad/hour, gray/hour, roentgen/hour, etc.
The EPA guidelines contained in Protective Action Guides and Planning Guidance for Radiological Incidents (2017), should also be familiar to CBRN operators and Hazardous Materials Technicians and those unfamiliar with them should remedy that situation. While the guide contains lots of information, most CBRN Operators and emergency responders need to remember only three numbers: 5, 10, and 25 rem (for the metric minded: 50, 100, and 250 mSv), as depicted in the chart below.

Here is where some confusion begins regarding alarm levels, turn back doses, and hotzone operations. Because these dose levels are in Rem or mSv, they do not readily translate to an alarm level for dose rate (there will be math involved, but don’t get scared by that, it is simple!). Most good monitors like the UDR-13 allow you to set dose and dose rate alarms. Dose alarms should, outside of emergencies, be set somewhere below five (5) rem to give operators a heads up and time to exit a situation before they cross the threshold (more on that below). In most cases its best to halve the dose limit you are using, so for emergency operations, the dose alarm rate is 2.5 rem (25 mSv) or lower. That means that if you took 2.5 rem (whole-body gamma) on the way in, you’re likely to take the same on the way out and emerge at or below the dose limit set in your operations planning or SOP.
It does not require complicated math to calculate dose rates, but it is a little tricky. For routine CBRN missions where radiation is present, the “occupational” dose limit of 5 rem per year (see the Maximum Permissible Dose Equivalent for Occupational Exposure chart below for more information) is too high. You should not get such high acute doses, and again – YOU NEED TO TRACK YOUR DOSES!
So, if it’s not an “emergency” or mission-critical task, figuring out dose rate and dose alarms is more complicated than a simple emergency dose of 5 rem/mSV. While you can set a dose alarm on equipment, the dose limit does not always convert easily into dose rate limit. You calculate REM doses based on if they are localized (in a particular spot – say the hands) or whole-body and the limits vary according to each.
Further, different radiations (alpha, beta, gamma, and neutron) have various conversion factors from dose rate to rem. While specialized CBRN operators and teams may have a health physicist or occupational safety specialist in their unit or can consult one remotely, not everyone is so lucky. Most regular CBRN and military units do not possess such expertise. That fact is a good reason for CBRN units and CBRN NCOs to liaison with supporting medical units, in addition to coordinating the possible medical evacuation of contaminated casualties before the mission.
There is a back of the envelope conversion CBRN Operators should remember that works for whole-body gamma radiation doses only. Since in most operations, gamma radiation is the primary concern because alpha and gamma are “point sources” (localized doses), the following is a “good enough” mnemonic to commit to memory (as long as its properly understood to apply to gamma only):
1 rad = 1 Roentgen = 1 Rem = 1 centiGray = 10 milliSievert
So, if 5 rem is the extreme upper dose limit (you will use something lower for routine missions, see discussion below), then working backward the operator should determine time on target (ToT) in hours, toss in a safety factor, and set their alarm. For example, if ToT is 2 hours and it is an “emergency,” or “critical” mission, then we could say 5 rem (50 mSv/5 cGy) divided by 2 equals 2.5 rem (25 mSv/2.5 cGy) per hour. For gamma radiation that converts one to one so set the alarm at 2.5 rad (2.5 cGy) per hour. However, we want to safe-side that a little, depending on how much we think the ToT might stretch. Therefore, we might pick an alarm level between 1 and 2 rad (1 or 2 cGy) per hour and a dose alarm of 2 or 2.5 (or lower). It is important to coordinate your dose and dose rate alarms when doing your mission planning for missions where you expect radiation. You need to know when the rate is climbing, and you need to know when your total dose is getting close to “time to leave” levels.
As mentioned above, CBRN units must track individual doses and make sure a system is in place before any operations and they must maintain and use it beyond their unit so that transfers of personnel come and leave with dose information from other units. For example, operators and the unit must recognize that a 5 rem/5cGy mission exposure excludes the exposed from radiation exposure for at least a year following the mission unless required by military necessity or other emergency conditions. Failure to track individual and unit doses violates all sorts of regulations, rules, laws, and other career-ending disasters, not to mention elevated health risks for all of those you fail to track.
For most military CBRN units, compliance with DODI 6055.08, Occupational Ionizing Radiation Protection Program and related service doctrine (Army, Navy, or Air Force) are mandatory except in emergencies and during combat or wartime military operations under the parameters specified in JP 3-11. Most civilian organizations will use the EPA and OSHA Guidance (or applicable NFPA standards where they apply due to contract or state/local regulation). The OSHA guidance and rules vary by industry and other factors, see the OSHA Ionizing Radiation Website for more information.
Certain US military CBRN units required to track radiation doses as part of their ordinary business usually have field dosimetry systems in place to do so. Those that do not and need to begin such tracking should consult their respective Service Dosimetry Center:
US Army Dosimetry Center, ATTN: AMSAM-TMD-SD, Building 5417, Redstone Arsenal, AL 35898-5000, Phone: 256-876-1786, Fax: 256-876-3816
US Air Force Radiation Dosimetry Laboratory, 2510 5th Street, Area B, Building 0840, Wright-Patterson Air Force Base, OH 45433-7212, Phone: 937-938-3764/1-888-232-3764, E-mail: esoh.service.center@us.af.mil
Naval Dosimetry Center, Walter Reed National Military Medical Center, 8901 Wisconsin Avenue, Bethesda, MD 20889-5614, Phone: 301-295-5410, Fax: 301-295-5981
The EPA/OSHA occupational exposure guidance uses safe sided numbers for the most basic non-emergency situations. While less desirable from a personal perspective, military and emergency needs outweigh such safety concerns, which is where the “emergency response” numbers of 5/10/25 come from in the EPA guidance. Most current military and intelligence CBRN operations involving radiation will happen below the 5 cGy/5 rem occupational limit and fall under the DODI 6055.08 or related service-specific guidance. The Joint Publication 3-11 Operations in Chemical, Biological, Radiological and Nuclear Environments, which conforms with NATO STANAGs applies to all military operations, including those above the 5 cGy/5 rem limits. However, the military must plan to operate in highly radioactive environments on the nuclear battlefield, where such safety limits quickly become impracticable.
While the new joint (and its corresponding service-specific) doctrine is a significant departure from some of the limits used in 2003/2004 when CBRN officers consulted the old FM 3-3-1 Nuclear Contamination Avoidance and set ridiculously high exposure limits, the new doctrine does not eliminate some of the issues with previous guidance. I discuss that in more detail below. For non-US CBRN operators, the NATO STANAGs related to JP 3-11 are STANAG 2473: Commander’s Guide to Radiation Exposures in Non-Article 5 Crisis Response Operations and STANAG 2471 Edition 4, Chemical, Biological, Radiological, and Nuclear (CBRN) Hazard Management for Airlift Operations. Additional guidance is in the NATO Allied Medical Publication (AMedP)-6(C) Volume 1: NATO Handbook on the Medical Aspects of NBC Defensive Operations (Nuclear) (NOTE: NATO classified the latest versions of these, they are not publicly available, but NATO members will find them referenced in their country’s military guidance and doctrine). See also references at the bottom of this article/page.
The JP 3-11 radiation guidance, which is in Appendix C of JP 3-11, is more complicated than the more straightforward EPA/OSHA limits above, but astute observers will note they conform to the EPA/OSHA limits at the lower end of the spectrum (similarly, much of DODI 6055.08 parallels OSHA occupational protection standards). However, military operations in radioactive environments may include actions on a nuclear battlefield, and therefore the guidance must account for situations that civilian and occupational limits do not deal with (another difference between CBRN and HazMat).
JP 3-11 outlines two different Operational Radiological Risk Management Tools: Radiation Exposure Status (RES) categories and Operational Exposure Guidance (OEG) levels. JP 3-11 specifies the application of the ALARA principle (as low as reasonably possible) in radiation operational risk management. The RES categories are an easy method for units to track dose and the associated operational impacts of radiation at a unit level. Units should not use RES categories for individual tracking except in the most extreme cases.

The average total cumulative dose received by a group is the basis for the RES Levels, calculated either from dosimetry data or estimated based on radiation monitoring data and total exposure time (see JP 3-11, Appendix C, page C-14 and related service doctrines for a complete description of the process). Each RES category has recommended actions that are cumulative at each level. The RES Levels divide into two further categories: Military Operations Other than War (MOOTW) and Military Operations During Combat. One of the problems with this system is that these two categories are not well defined in doctrine and may prove confusing to the average CBRN Officer or NCO, as many MOOTW include combat and some operations in “combat” zones probably ought to use the MOOTW category.
The second system, Operation Exposure Guidance (OEG), is even more subjective, though it features more exposure limit gradients. According to JP 3-11, the OEG is set for each platoon or equivalent unit and for each mission. It requires the commander’s evaluation, based on guidance from supporting staff, of three variables: Severity of the Radiological Threat, Probability of Radiological Threat, and Mission Importance. The problem with this ought to be evident to anyone with military operations experience. Commanders tend to define ALL their missions as critical, and CBRN officers/NCOs tend to “worse case” things, thus elevating the severity of the threat, probability of the threat, and mission importance beyond reasonable levels. Common sense is seldom common, especially in technical topics that carry with them inherent fears and misconceptions. It was precisely this reason that both the First Gulf War and Operation Iraqi Freedom saw units with such insane exposure guidance.
Further, while doctrine specifies to set the OEG at a platoon level for each mission, it doesn’t state who sets the limit, only for whom the limit is set. Most non-CBRN (and more than a few CBRN) platoon leaders are ill-equipped and lack the knowledge and support structures to evaluate and set such limits on their own. Worse, higher levels of command, which have access to more knowledgeable advisers, might set blanket levels for subordinate units that violate the “platoon level” dictate, or set theater or command levels in blanket operations orders that obliterate the “per mission” guidance.
Still, despite my reservations about this system, it is better than what it replaced. However, it is not the greatest for everyone. Because it is doctrine, many CBRN professionals need to know, understand, and practice it, and it is worth reviewing. However, I challenge each of you reading this to share your knowledge about the system and teach others how to apply the OEG system appropriately. Only then can we overcome its shortcomings.
To begin setting an OEG, a commander needs to define the platoon (or equivalent) mission importance. JP 3-11 describes three (somewhat subjective) levels of mission importance. I caveat the doctrine with this personal observation: Beware of mission criticality inflation!
Critical missions are essential to the overall success of a higher headquarters’ operation, emergency lifesaving missions, or the [undefined] equivalent.
Priority missions avert danger to persons, prevent damage from spreading, or support the organization’s mission-essential task list (METL).
Routine missions are all other missions not designated as priority or critical missions.
I don’t know what you think, but I see that all as vague and problematic and the inclusion of METL makes it highly suspect. Does any military unit conduct missions that don’t in some way involve their METL? Further, if a mission isn’t essential to overall success, is it even worth doing? Herein are the problems.
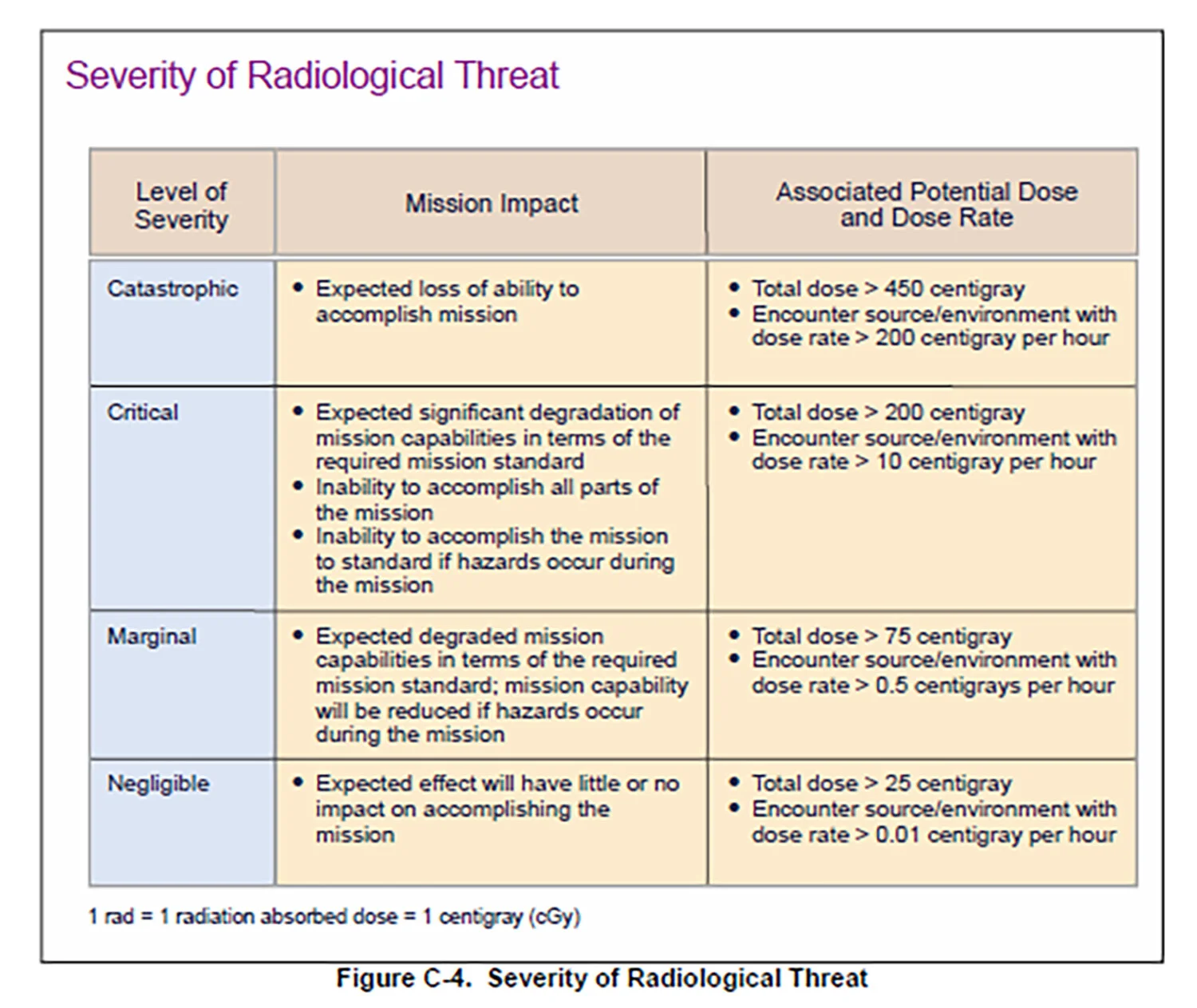
The second step is assessing the Severity of Radiological Threat. Here is where we have a massive threat inflation problem. Right now, there are bone-headed individuals in CBRN shops that are going to always go with “Catastrophic” or “Critical,” because “nuclear bombs could happen.” Not that they are at all likely, mind you, but it could happen, so the severity is always turned to eleven in every scenario they imagine. You know that guy, I know that guy, and he’s the same guy that writes those horrible exercise scenarios with the Anthrax/Sarin/RDD bombs we all love to hate. In any case, if we’ve got someone who is more in touch with reality evaluating the threat severity based on something like actual intelligence about the threat, target, and route of march, then they do so based on a single parameter, Mission Impact which is based on an Associated Potential Dose and Dose Rate (see chart below).
So, looking at the Severity of Radiological Threat chart below, you see the doses are all above the OSHA/EPA emergency limits, with 25 cGy being “negligible” severity. There is some mismatch in the way the guidance uses this terminology, and it is going to confuse some folks. Again, I digress.
Next, the commander (at an indeterminate level of command at or above the platoon) and his advisors (if he has them) assess the Probability of Radiological Threat. This category puts some boundaries on the assessment and gives some odds, though the odds seem wildly out of sync with the descriptions. For example, the “frequent” probability is defined as a 1 in 500 likelihood but then described as “expected to occur several times or continuously over the duration of a specific mission.” I don’t know in what universe a 1 in 500 chance of something is frequent. Even casinos don’t have such bad odds. Worse, the description and the probability are entirely “at odds” with one another, but I’m digressing again, this time with bad puns.

The next step is an assessment of the level of Radiological Risk. We take our Severity and Probability and get a level of radiological risk on the chart below. This chart gives us a Mission Radiological Risk. The OEG is set based on “Acceptable Risk Level” versus “Mission Importance.”
Mission Risk and Acceptable Risk are two different things and the confusion of them between the text and the charts in JP 3-11 is another problem with this system, but if someone reads the text of JP 3-11 instead of just looking at the pictures they will see it advises “begin by selecting a conservatively low OEG” and reassessing based on mission impact using the Recommended Operational Exposure Guidance levels and only raising the levels if the mission impact and mission criticality require it.
An experienced CBRN professional will only need to look at Figure C-7 in JP 3-11 (below) to see the levels are safe sided for most missions and set their OEG accordingly. IMHO, the key to making the JP 3-11 system work is keeping that “worst-case” guy away from it. (As an aside: the entire process of using multiple charts to set an OEG feels like something a fan of certain role-playing games devised, I almost expected to see a 20-sided dice involved in the process).

JP 3-11 also notes risk mitigation - something I want to stress and talk about at more length in a few minutes when I talk about time, distance, and shielding. JP 3-11 adds three other radiological risk mitigation factors worth noting: Avoidance, PPE and Collective Protection (COLPRO) that controls contamination risks and limits internal contamination, and Decontamination, all of which can play an essential role in mission planning that may reduce the necessity to set a higher limit. As JP 3-11 also notes, each of these may increase other risk factors, for example, avoidance of a radiologically contaminated area may channel your unit into a kill zone. Likewise, decontamination may take you out of the fight and poses containment and disposal problems for radioactive materials.
In other words, the OEG process and risk mitigation factors make for a complicated process, too complicated for most military units. CBRN folks need to study up on these and get familiar with them if they hope to advise commanders and units on setting realistic OEGs.
Radiation in Mission Planning
As seen in the above discussion, there’s a lot to take in when trying to set dose and dose rate exposure levels and so-called “turn back” doses. It is not as easy as just picking a number off a chart; there is so much more to consider. I’m going to circle back to that later in this post, and as part of a broader post about CBRN Operations Planning, down the road. For now, that’s enough. I’m not even going to touch the different radiation exposure standards in different countries, militaries, treaty organizations, and the IAEA – you can explore those on your own, I’ve listed some sources at the bottom of this post/article.
Just remember, even the emergency 25 rem/25 cGy dose levels do not pose massive long-term risks in the general sense. They are not desirable, but a onetime acute dose of 25 rem is not likely to kill you even in the long term. Smoking a giant Cohiba and downing a bottle of Scotch after every mission might be more harmful in the long run. Even higher doses of radiation are not immediately lethal (hence their use in the old Cold War FM 3-3-1), though they tend to increase the risk of latent effects (cancer, leukemia, etc.). So, a single dose of 100 rem is survivable, but may have long term effects and significantly increase leukemia risks.
That doesn’t mean a 25 rem/25 cGy dose is not without problems: a 25 rem acute dose can produce temporary sterility in men, but there are long-running scientific debates about the long-term at lower exposure levels, and such studies are not conclusive as to the long term health risks of low-level radiation exposure. Also, important to note is that most of these limits originally developed out of studies looking at military-age males. Even low radiation doses, like disease and chemical exposure, produce more noticeable effects on infants and children, the elderly, and pregnant women, whereas low-level whole-body doses show less risk for healthy adults. Again, the levels may not account well for differences between genders a problem with a lot of the exposure guidelines and not just for radiation (but that’s also a topic for another day).
For those who’ve forgotten the effects of radiation at different dose levels, based on military-age males, (this is Cold War testing data we are talking about) it is as follows:
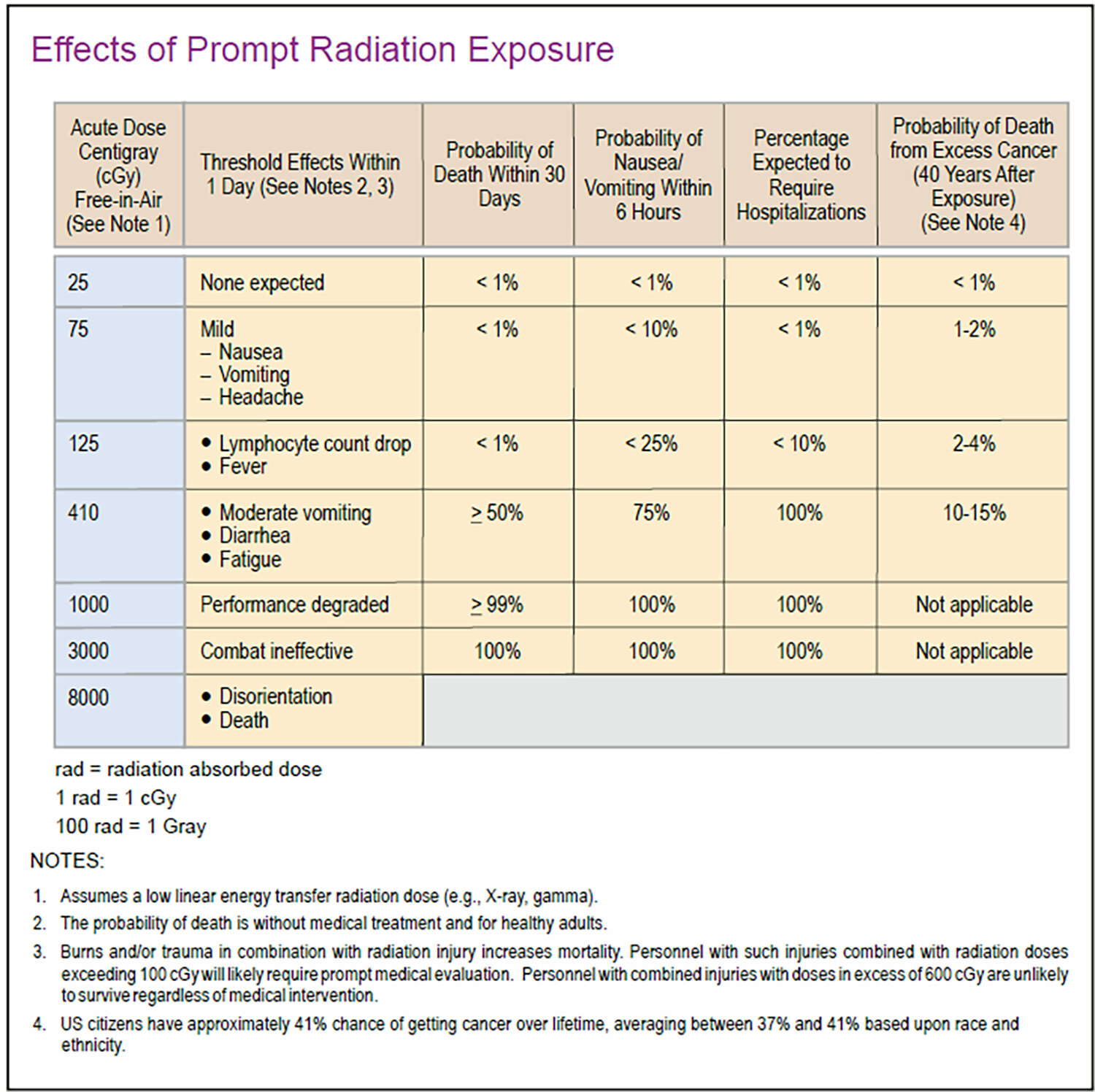
Source: Joint Publication 3-11 Operations in Chemical, Biological, Radiological and Nuclear Environments, See also Department of the Army Pamphlet No. 50-3: The Effects of Nuclear Weapons (March 1977) for more detail.
The main point is that a little bit of radiation will not kill you. Still, CBRN professionals must deal with inherent (and often irrational) fears most of the population have regarding radiation, even among those who ought to know better. That means that leaders of CBRN professionals must incorporate education and training for their personnel beyond providing dose and dose rate limits for operations. Soldiers and CBRN professionals often have the same doubts and fears as the general public about radiation and may be distrustful of any limits passed from on high.[3] It is therefore extremely important that CBRN professionals educate themselves and others regarding the “whys” behind any limits they establish, and they must know when to question them if they don’t track with reality. A CBRN professional that remembers the 5, 10, 25 rem numbers but does not know the reasoning behind them is not adequately trained!
I offer just one, last point on radiation exposure, dose, and mitigation: ALWAYS REMEMBER TIME, DISTANCE, AND SHIELDING. The basic rules regarding measures to reduce exposure can allow operations to continue safely, even in areas where there are elevated levels of radiation. They do require a bit of ingenuity, however. During training iterations, I’ve witnessed CBRN teams hit a dose or dose rate alarm and evacuate a site they were supposed to exploit for non-radioactive materials and reasons. Instead of re-evaluating ways they might still accomplish their mission, they abandoned it. Other teams hitting the same scenario moved to a safe distance, re-evaluated their approach and re-entered to achieve their task at safe dose and dose rate levels. The ability to make such calls comes from training, education, and experience.
Take the following example: entering a site where radiation is unexpected, radiation alarms go off shortly after a search team enters a laboratory. Moving to a safe distance, the team looks around the site and using their monitors and detectors determines that the source of the radiation is in one corner of the lab. The unit uses the “double the distance, quarter the dose” rule to calculate a safe distance from the source and the team leader marks it on the floor or verbally cautions the team members where to avoid entering, allowing the team to exploit the rest of the room before returning to the question of the source and its purpose. Attaching a detector to a broom handle found on-site, they stand safely at a distance from the source while using a ballistic shield retrieved from a truck outside for additional shielding that lowers their dose further. The combination of time, distance, and shielding allow them to safely find the exact source of the radiation and identify it as an open pig in the corner of the room. To further limit the dose, the team each take turns using their broom handle detector and holding the shield (reducing the time of exposure). They deploy an EOD robot to replace the pig’s cover, retrieve the pig, and the team departs the site with the source safely contained, taking it with them. They accomplish both their original mission (exploiting the lab) and one they never expected (securing a loose radiation source).
There are many such scenarios, and CBRN teams should practice against them. Leaders should encourage and reward improvisation and ingenuity in such cases and allow for it in their exercise scenarios. Such things have no right answers but frequently have better ones than a simple “go/no go” criteria allows. It is usually best to repeat training iterations across changing scenarios and enable individuals to develop solutions on their own rather than trying to teach them directly. Let the AAR do the teaching. Have teams talk to one another about how they solved the problem, then revisit the scenario and work out a “best practice” for everyone that incorporates that learning. Practicing and developing the skill sets that increase personnel safety requires flexibility and adaptability that is not easy to create, especially in hierarchical organizations, but it is essential to safety. The most effective protective equipment CBRN professionals possess is between their ears.
In my next post, I’ll close out the Basic Kit with an extended examination of confined space monitors, understanding the data they provide, how to use them correctly in combination with a PID, and methods for establishing safety criteria based on PPE and target information that CBRN operators can incorporate into their Safety Plans and SOPs. Until then remember, no matter what situation you find yourself in as a CBRN operator: Keep Calm and Decon.
References:
United States Army, Technical Manual 11-6665-364-12: OPERATOR`S AND UNIT MAINTENANCE MANUAL FOR RADIAC SET AN/UDR-13 (W/BASIC INCL C1-2), (NSN 6665-01-407-1237). Available to authorized users at https://armypubs.army.mil/ProductMaps/PubForm/Details.aspx?PUB_ID=76799
United States Department of the Army, Pamphlet No. 50-3: The Effects of Nuclear Weapons (March 1977).
United States Department of Defense, Joint Publication 3-11 Operations in Chemical, Biological, Radiological and Nuclear Environments.
United States Environmental Protection Agency, Protective Action Guides and Planning Guidance for Radiological Incidents (2017).
United States Nuclear Regulatory Commission, US Code of Federal Regulations, 10 CFR 20.1201, Subpart C, Occupational Dose Limits for Adults, https://www.nrc.gov/reading-rm/doc-collections/cfr/part020/part020-1201.html
NATO and Allied Nation References:
UK Civilian Radiation Occupational Exposure Limits: http://www.hse.gov.uk/radiation/ionising/doses/index.htm
UK Civilian Emergency Radiation Exposure Limits: http://www.hse.gov.uk/radiation/ionising/reppir.htm
UK Ministry of Defence (MoD) Management of radiation protection in defence (JSP 392): https://www.gov.uk/government/collections/jsp-392-radiation-safety-handbook
IAEA Safety Standards: https://www.iaea.org/resources/safety-standards/search
EU Radiation Protection (General): https://ec.europa.eu/energy/en/topics/nuclear-energy/radiation-protection see also https://osha.europa.eu/en/legislation/directives/directive-2013-59-euratom-protection-against-ionising-radiation
EU Dosimetry Program Recommendations: https://ec.europa.eu/energy/sites/ener/files/documents/160.pdf
This webpage lists the emergency dose limits for Canada, France, the Republic of Korea (South Korea), and Russia (in English) as of the date of publication: https://www.ilo.org/safework/whatsnew/WCMS_154370/lang--en/index.htm
France Occupational Exposure Limits: https://www.irsn.fr/FR/professionnels_sante/radiopro_travailleurs/Pages/rad_travailleurs_siseri.aspx#.XWaI_igzaUk
Japan Nuclear Regulation Agency (in English): https://www.nsr.go.jp/english/ (in Japanese): https://www.nsr.go.jp/
German Radiation Exposure Limits (in German): https://www.bfs.de/DE/themen/ion/strahlenschutz/grenzwerte/grenzwerte.html
Czech National Radiation Protection Institute (in English): https://www.suro.cz/en (in Czech): https://www.suro.cz
Czech Military Research Institute State Enterprise, CBRN Protection (in English): https://www.vvubrno.cz/en/cbrnp/
[1] The Army will field two new RADIAC and dosimeter systems in coming years: the Radiological Detection System (RDS) that will replace current survey meters and RADIAC devices (mostly AN/PDR-77 kits) and the Joint Personal Detector (JPD), a wrist mounted dosimeter that replaces the UDR-13. Both incorporate lessons learned from US support to Japan in the Fukishima disaster (Operation TOMODACHI).
[2] From the 1970s until quite recently any radiation (exposure, not contamination) over normal background, according to the old EPA definition of a public health risk, even at extremely low levels, was a threat. As many pointed out during that period, that meant that someone living in New York City (at sea level) might have a public exposure limit that was below the normal background radiation in Denver, where, due to elevation, background is about three times higher. EPA, after years of urging, finally re-examined its criteria and made modest improvements, though their new guidance remains a point of contention.
[3] Not all of which are unjustified. After all, CBRN officers setting limits based on Nuclear Contamination Avoidance Field Manual guidelines in Iraq 2003-2005, were wrong and deserved to be questioned, as were the many units that pre-administered pyrostigmine to units during the first Gulf War despite the fact there was no evidence of Iraqi Soman production, thus creating many of the most severe cases of the so-called “Gulf War Syndrome.”



